
Intimate Partner Violence Among Same-Sex Relationships
Program Vision and Health Objective
We envision a world free of intimate partner violence within the LGB community. Our program’s primary goal is to decrease the incidence of intimate partner violence within the LGB-identified community in Washington, D.C.
Background
According to the World Health Organization (WHO), intimate Partner Violence (IPV) is violence or aggression that occurs in a close relationship (2012). It involves acts of physical, sexual, emotional, controlling behavior or psychological harm by a partner [Centers for Disease Control and Prevention (CDC), 2018] (see Figure 1). Regardless of gender, age, marital status or sexual orientation, IPV is about power and control (The National Domestic Violence Hotline, 2019). IPV in same sex couples poses a great public health concern due to the high number of individuals affected and the threats posed onto an individual’s health. There is an estimated higher prevalence of lifetime experiences of IPV among bisexual women than heterosexual women and bisexual men seem more likely to report having experienced IPV than heterosexual men (Smith, 2019). It has been reported that 26.9% of gay men experienced IPV in their lifetimes and 12.1% gay men had experienced IPV in the past year. An in-depth view of the quality of life, risks, health consequences, and several correlated factors, is needed to understand the severity of IPV. There are severe consequences to individuals who experience IPV, including several health conditions, reproductive, psychological and social issues (“Consequences: Intimate Partner Violence” (n.d), 2019).
Get Help With Your Essay
If you need assistance with writing your essay, our professional essay writing service is here to help!
In addition to an individual’s struggles with IPV, there are costs associated for the society. It has been shown that the lifetime per-victim cost was $103,767 for women and $23,414 for men. For the U.S. population, the lifetime cost is $3.6 trillion (CDC, 2019). The focus of research on this population and IPV is important, because it was estimated that 3% of the total research on IPV was dedicated to the LGB community (Edwards, Neal, & Sylaska, 2015).
Social Assessment
Among the LGBT community, the highest number of couples per one thousand households is in D.C. with approximately 18.8 couples per 1,000 households (“Same-sex Couple Data & Demographics – The Williams Institute,” n.d.). In D.C., the LGBT community makes up 10.8% of the total population and 68% identify as females and 32% identify as males. Also, individuals reported themselves as 53% White, 31% African American, 6% Hispanic and 6% as other race. The average age of individuals in same-sex couples is 36.7 years old. According to the 2017 Washington, D.C. LGBT Health report, 58.9% of the LGBT population in D.C. is a college graduate, 63.6% of LGBT in D.C. have an income of $50,000 or more (D.C. Department of Health, 2017). Additionally, 13.4% of LGBT in D.C. could not see a doctor in 2017 because of the cost, and 95.5% of LGBT in D.C. have health insurance, compared to 92.3% non-LGBT
Quality of Life
The LGB population faces more complex outcomes in comparison to the heterosexual population relating to mental and physical health, subjective well-being, employment opportunities, socioeconomic status, housing, and community inclusion (Perales & Todd, 2018). While research on IPV among the LGB is still sparse, IPV is the third largest problem faced by gay men, following AIDS and substance abuse. IPV has been linked to substance abuse among men who have sex with men (MSM), as well as high-risk sexual behavior and mental health issues (Arnett, 2000). Additionally, emotional, physical, and sexual abuse among same-sex partners has led to severe outcomes such as physical injury, social isolation, property loss and/or destruction, disturbances to work, education, and advancement of career (Barrett, 2015).
According to the 2017 Washington D.C. LGBT Health Report, LGBT adults were more likely than their non-LGBT counterparts to report 15-30 days of mental health not
being good, which includes stress, depression and problems with emotions (DC Department of Health, 2017). Further, the report noted that LGBT adults were more likely than their non-LGBT counterparts to have engaged in high risk behaviors such as unprotected anal sex, thus increasing their risk for HIV infection. Additionally, LGBT adults in D.C. were more likely than non-LGBT adults to be treated for a STD within the past 12 months, use drugs recreationally in the past 12 months, and had sex with a partner other than a primary partner within the past 12 months. The
report also mentioned D.C. LGBT adults were more likely than their non-LGBT counterparts to be diagnosed with asthma and depressive disorder. These findings indicate that the challenges in health outcomes among sexual and gender minorities in D.C.
In addition to physical and mental health outcomes, cultural gender norms also impact quality of life. Culturally conceived beliefs on masculinity and femininity may diminish the seriousness of IPV within the LGB population, particularly the traditional heterosexual relationship power dynamics, where the male partner in the relationship is the “partner in control” (Johnson, 2006). Gender theories are usually used to analyze the occurrence of IPV, but when there is an absence of a male perpetrator, IPV may be harder to explain (Kimball, 2001). Stereotypes like lesbian IPV is “harmless because women are not physically strong and dangerous,” or that “homosexual men are less masculine than heterosexual men” are detrimental to the way a community responds to LGB-related IPV–hindering victims from coming forward (Ristock & Timbang, 2005).
Epidemiologic Assessment
The 2010 National Intimate Partner and Sexual Violence Survey (NISVS) reported that an estimated 37.3% and 25.2% reported lifetime intimate partner violence among bisexual and gay men, respectively (Walters, Chen, & Breiding, 2013). Also, an estimated 56.9% and 40.4% reported lifetime intimate partner violence among bisexual and lesbian women, respectively.
Biological & Genetic Determinants
Biological and genetic factors may predict greater risk of IPV among same-sex couples. A study examining a sample of hazardous drinking men in batterer intervention programs in Rhode Island found that there are genetic causes to IPV (Stuart, McGeary, Shorey et al, 2014). It was found that a cumulative genetic score (CGS) containing monoamine oxidase A (MAOA) and the human serotonin transporter gene polymorphisms (5-HTTLPR) are significantly associated with physical, psychological aggression and violence resulting in injuries to partners. This association was found after controlling for effects of alcohol and drug problems, age, and relationship length. In addition to specific genetic variation, biological determinants are found to be causes of IPV.
A study investigated and collated sex differences in aggression between heterosexual partners across time in the United States (Archer, 2000). Researchers found that women were more likely than men to use one or more acts of physical aggression and more frequently. Men were more likely to inflict injury. Also, 62% of women reported being injured by a partner.
Heredity has influenced sexual crime and aggression and a 37-year long study examined longitudinal, nationwide Swedish crime and multigenerational family registries to examine the relationship between sexual crime and biological influences (Långström, Babchishin, Fazel et al, 2015). Men included in the study were convicted of any sexual offense, including many who committed rape of an adult and child molestation. The study found strong evidence of familial clustering of sexual crimes among full brothers of convicted sexual offenders. Furthermore, genetic factors accounted for 40% of the sexual crime, while non-shared environment accounted for 58% and shared environmental influence accounted for 2%. A twin study demonstrated that shared genes explained familial resemblance in psychological and physical intimate partner aggression (Hines & Saudino, 2004). The analyses found that heredity accounts for a significant proportion and suggests a genetic predisposition to get involved in aggressive relationships.
The overall results showed a strong association of genes, rather than environment, demonstrate a causal relationship between genetics and sexual violence. (Långström, Babchishin, Fazel et al, 2015, Hines & Saudino, 2004)
Behavioral Determinants
Many behaviors applicable to the LGB community within the D.C. can enhance and/or reduce the risk factors for IPV. A number of studies that highlight IPV in LGB communities within different cities of the United States carry similar behavioral causes that can help better understand our target population. A lack of trust is one behavior that increases the risks for IPV. For instance, a survey of 1,075 men from Atlanta who had identified as gay or bisexual were asked a series of questions that highlighted the potential triggers for IPV. Nearly 85.6% of those who had a recent experience of IPV believed a lack of trust between partners “possibly can” or “definitely will” cause IPV (Finneran, 2014).
Unsafe sexual activity is another behavioral factor that can magnify the risk for IPV. Within the same study of gay and bisexual men who had a recent experience of IPV, 62.5% believed it to be due to disagreements about sex. This ranged from sex frequency to more specifically determining who was the insertive versus the recipient partner during anal sex (Finneran, 2014). Condomless anal intercourse (CAI) was measured and assessed among the participants. It was found that “men who reported recent experience of physical or sexual IPV had significantly higher odds of reporting CAI” (Stephenson, 2017). Gay and bisexual men who engaged in unsafe sexual practices (such as unprotected anal sex) were also more likely to be involved in a violent relationship (Ard, 2011).
Another behavioral factor that can increase the likelihood of IPV is engaging in alcohol/substance abuse. A survey conducted in New York City with 226 MSM to determine whether their alcohol use was linked to their experience of IPV. An Alcohol Use Disorders Identification Test was conducted to measure alcohol dependence and related-issues. Over 54% experienced one form of IPV within the past year by a partner, whereas 48.7% admitted to engaging in IPV against their partner. Higher levels of alcohol use were determined to have strong associations “in the perpetration and victimization of both physical/sexual and psychological forms of IPV in male–male intimate relationships” (Davis, 2016).
Substance abuse is another behavioral measure that can increase the risk of IPV within the LGB community. A survey done in Boston, Massachusetts, sampled 3,103 LGB patients at a medical care center that assessed their substance abuse and IPV history. About 17.1% had a history of consuming either “alcohol, cocaine, heroin, injection drug use, or other recreational drugs” (Reisner, 2013). Substance abuse-related IPV was highly associated for both males and females in the study with “lesbian-identified women having 2.2 times the odds and bisexual women having 2.3 times the odds of lifetime substance misuse compared to heterosexual female patients” (Reisner, 2013).
Methods of coping within the LGB community can also impact couples that deal with IPV. In a national online survey conducted by Virginia Commonwealth University, 89 sexual minority men (gay, bisexual, queer, and “other” non-heterosexual orientation) were selected and asked a series of questions to better understand their experience in dealing with IPV through positive and negative coping styles. The study found that repeat offenses of IPV was directly impacted by coping styles that engaged in denial, religious coping, and behavioral disengagement. However, it was lessened with active coping, positive reframing, acceptance, and planning that entailed “creating a safety plan to protect oneself from the abuser, making plans to leave the abuser, or storing an emergency fund outside of the home to ensure financial stability” (Goldberg-Looney, 2016).
Environmental Determinants
There are many environmental determinants that negatively impact the LGB community and feeds into the previously discussed behavioral factors, health outcome, and overall quality of life. A major factor affecting the service environment of the LGB population within D.C. is the severe inequality and accessibility of emergency housing. The majority of emergency housing and domestic violence shelters only admit female survivors to create a “safe place” for heterosexual women seeking protection from abusive male partners (Simpson & Helfrich, 2007). According to the District Alliance for Safe Housing, “Though there are no domestic violence housing programs that are specifically for LGBTQI survivors in DC, two programs in Maryland state that they serve LGBTQI survivors” (2019).
Find Out How UKEssays.com Can Help You!
Our academic experts are ready and waiting to assist with any writing project you may have. From simple essay plans, through to full dissertations, you can guarantee we have a service perfectly matched to your needs.
View our academic writing services
Lesbian survivors expressed fear of homophobic attitudes held by heterosexual shelter residents (Simpson & Helfrich, 2007). Heterosexual shelter residents displayed a resistance to accept or interact with lesbians, presumably for fear of being sexually propositioned. Consequently, heterosexual women refused to share rooms or spaces with lesbian residents because they were preoccupied with lesbian survivors’ sexual orientation, rather than their shared experience of surviving relationship violence (Simpson & Helfrich, 2007, p. 52). Other lesbian survivors reported agency staff lacked the education and experience of working with lesbian survivors and tended to make discriminatory remarks (Simpson & Helfrich, 2007).
These factors left bisexual and gay men without a support network meant to prevent Intimate Partner Violence. Additionally, bisexual and lesbian women felt unsafe or unwelcome, preventing resource utilization and forcing them to stay in an unsafe environment. To compound these problems, motivating the domestic and intimate partner violence response community to adopt the issue is difficult because of practical barriers related to insufficient staffing and funding, resulting in unsustainable programs and nearly zero push for policy changes (Rogers, 1999).
Educational and Ecological Assessment
Predisposing factor for IPV among LGB include stigmatization and internalized homophobia. Stigmatization, the simultaneous acts of labeling, stereotyping, separation, loss of status, and discrimination, leads to limited access to resources and opportunities (such as employment and healthcare), which then lends to social isolation, causing stress, and can ultimately result in a maladaptive coping method, a behavioral determinant for IPV (Hatzenbuehler, Phelan, & Links, 2013). This perceived discrimination among minority group members has been linked to health problems, such as adverse psychological responses (Meyer, 2003). As stated in the 2013 National Intimate Partner and Sexual Violence Survey, 4.1 million people of the LGB community (sexual minority men and women) in the United States have experienced IPV in their lifetime (Walters, Breiding, & Chen, 2013).
Internalized homophobia is the extent to which individuals within a sexual minority have internalized negative feelings, attitudes, beliefs, behaviors, and assumptions about their homosexuality (Balsam, 2001). Multiple studies have indicated that internalized homophobia could be associated with violent behavior against one’s own group member (Renzetti, 1998). Additionally, eight studies have shown positive and statistically sound associations between internalized homophobia and IPV perpetration and victimization, demonstrating that higher levels of internalized homophobia were related to higher levels of IPV (Rentezzit, 1998).
Further stigmatization within healthcare may be enabling forces for IPV among LGB. Several studies have indicated that health professionals who conducted IPV assessments for heterosexual female patients did not normally provide the same screening for lesbian or bisexual female patients or male patients of any sexual orientation (Barata, Fante-Coleman, Furman et al, 2015, Messinger, 2011). The assumptions that violence among same-sex partners may not be as severe as heterosexual cases, that the perpetrator is always a man and the victim is a woman, and/or that it’s easier for LGB individuals experiencing IPV to leave the abusive relationship has perpetuated the healthcare inequality and improper responses from community members and law enforcement (Merrill & Wolfe, 2000).
A reinforcing factor to IPV within the LGB population is the victim/abuser reliance. According to “An Exploration of Abuse,” both heterosexual and homosexual victims frequently listed love for the partner, financial and emotional dependency on the partner (Merrill & Wolfe, 2000). This dependence allows the perpetrator to continue with the abuse, with minimal consequence. In addition to this, another reinforcing factor is the “invisible” issue within the community, as mentioned previously. There have been several common fears with the recognition of IPV within the LGB community (Ristock, 2003). The LGB community is used to further stigmatization of IPV in the community, which then contributes to continuous oppression and social marginalization. IPV has not been significantly researched or acknowledged by the public, thus there are limited consequences, so the behavior is perpetuated.
Summary
IPV is violence or aggression that occurs in a close relationship (WHO, 2012). It involves acts of physical, sexual, emotional, controlling behavior or psychological harm by a partner (CDC, 2019). Individuals who experience IPV may have several health issues, including reproductive, psychological and social ailments. IPV impacts LGB quality of life, including the following: poor health outcomes (Arnett, 2000), social isolation (Barrett, 2015), and disruption to work and career advancement (Pareles & Todd, 2018).
There are studied genetic, biological, behavioral and environmental determinants that cause IPV. The MAOA and the 5-HTTLPR polymorphisms are significantly associated with physical, psychological aggression and violence resulting in injuries to partners (Stuart, McGeary, Shorey et al, 2014). It was found that women were more likely to use one or more acts of physical aggression and men more likely to inflict injury, demonstrating differences in sex (Archer, 2000). Genetic factors account for 40% variance for sexual crime (Långström, Babchishin, Fazel et al, 2015). In a study of gay and bisexual men, nearly 85.6% believed alack of trust between partners could cause IPV (Finneran, 2014). Gay and bisexual men who practiced unsafe sexual activity were more likely to be involved in a violent relationship (Ard, 2011). Alcohol use and substance abuse had strong ties to IPV and perpetuating the victim (Davis, 2016, Reisner, 2013). Repeated acts of IPV was directly impacted by coping styles such as denial, religious coping, and behavioral disengagement, while IPV lessened with active coping, positive reframing, acceptance, and planning (Goldberg-Looney, 2016). Risk factors that are linked to minority stress and stigmatization contribute to a higher percentage of violence experienced by homosexual and bisexual couples (Messinger, 2011). To compound the multiple factors that contribute to IPV, there are several environmental factors that do not support healthy behaviors. The lack of emergency shelters and an unsupportive environment that surrounds them (Simpson & Helfrich, 2007) is only made worse by the lack of funding (Rogers, 1999).
A holistic examination of quality of life, correlated factors and the biological, behavioral and environmental determinants is necessary to prevent IPV within the LGB community.
References
- Ard, K. L., & Makadon, H. J. (2011). Addressing Intimate Partner Violence in Lesbian, Gay, Bisexual, and Transgender Patients. Journal of General Internal Medicine, 26(8),930–933. https://doi.org/10.1007/s11606-011-1697-6
- Arnett J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55, 469-480.
- Balsam K. F. (2001). Nowhere to hide: Lesbian battering, homophobia, and minority stress. Women and Therapy, 23, 25–38. doi:10.1300/J015v23n03_03
- Barata P., Fante-Coleman T., Furman E., Wilson C. (2017). “It’s a gap in awareness”: exploring service provision for LGBTQ2S survivors of intimate partner violence in Ontario, Canada. J. Gay Lesbian Soc. Serv. 29 1–16. 10.1080/10538720.2017.1365672
- Barrett B. J. (2015). Domestic Violence in the LGBT Community.Available at: http://socialwork.oxfordre.com/view/10.1093/acrefore/9780199975839.001.0001/acrefore-9780199975839-e-1133
- Centers for Disease Control and Prevention (2018, December 11). Summary and Special Reports. Retrieved January 29, 2019, from https://www.cdc.gov/violenceprevention/nisvs/summaryreports.html
- Consequences: Intimate Partner Violence. Violence Prevention and Injury Center, CDC. (2019, February 5). Retrieved February 18, 2019, from https://www.cdc.gov/violenceprevention/intimatepartnerviolence/consequences.html
- Davis, A., Kaighobadi, F., Stephenson, R., Rael, C., & Sandfort, T. (2016). Associations Between Alcohol Use and Intimate Partner Violence Among Men Who Have Sex with Men. LGBT Health, 3(6), 400–406. https://doi.org/10.1089/lgbt.2016.0057
- Domestic and Intimate Partner Violence: Gateway to Health Communication. CDC. (2018, March 28). Retrieved January 29, 2019, from https://www.cdc.gov/healthcommunication/toolstemplates/entertainmented/tips/Violence. html
- District Alliance for Safe Housing: I Am LGBTQI. (n.d.). Retrieved February 17, 2019, from https://www.dashdc.org/housing-resource-center/find-safe-housing/lgbtqi/
- Edwards K. M., Neal A. M., Sylaska K. M. (2015). Intimate partner violence among sexual minority population; A critical review of the literature and agenda for future research. Psychol. Violence 5 112–121. 10.1037/a0038656
- Finneran, C., & Stephenson, R. (2014). Antecedents of Intimate Partner Violence Among Gay and Bisexual Men. Violence and Victims, 29(3), 422–435.
- Goldberg-Looney, L. D., Perrin, P. B., Snipes, D. J., & Calton, J. M. (2016). Coping Styles Used by Sexual Minority Men who Experience Intimate Partner Violence. Journal of Clinical Nursing, 25(23–24), 3687–3696. https://doi.org/10.1111/jocn.13388
- Government of the District of Columbia. (2017). Report on the Health of the Lesbian, Gay, Bisexual, and Transgender (LGBT) Community in the District of Columbia. Retrieved from https://dchealth.dc.gov/sites/default/files/dc/sites/doh/publication/attachments/LGBT%20Health%20in%20the%20District%20of%20Columbia.pdf
- Hatzenbuehler, M. L., Phelan, J. C., & Link, B. G. (2013). Stigma as a fundamental cause of population health inequalities. American journal of public health, 103(5), 813-21.
- Hines, D. A., & Saudino, K. J. (2004). Genetic and Environmental Influences on Intimate Partner Aggression: A Preliminary Study. Violence and Victims; New York, 19(6), 701–718. http://dx.doi.org.proxygw.wrlc.org/10.1891/088667004780927729
- Hipwell, A. E., Stepp, S. D., Keenan, K., Allen, A., Hoffmann, A., Rottingen, L., & McAloon, R. (2013). Examining links between sexual risk behaviors and dating violence involvement as a function of sexual orientation. Journal of Pediatric and Adolescent Gynecology, 26(4), 212–218. https://doi.org/10.1016/j.jpag.2013.03.002
- Långström, N., Babchishin, K. M., Fazel, S., Lichtenstein, P., & Frisell, T. (2015). Sexual offending runs in families: A 37-year nationwide study. International Journal of Epidemiology, 44(2), 713–720. https://doi.org/10.1093/ije/dyv029
- Merrill G. S., Wolfe V. A. (2000). Battered gay men: an exploration of abuse, help seeking, and why they stay. J. Homosex. 39 1–30. 10.1300/J082v39n02_01
- Meyer, I. H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological Bulletin. 2003;129(5):674. http://dx.doi.org/10.1037/0033-2909.129.5.674
- Perales F., Todd A. (2018). Structural stigma and the health and wellbeing of Australian LGB populations: exploiting geographic variation in the results of the 2017 same-sex marriage plebiscite. Soc. Sci. Med 208 190–199. 10.1016/j.socscimed.2018.05.015
- Reisner, S. L., Falb, K. L., Van Wagenen, A., Grasso, C., & Bradford, J. (2013). Sexual Orientation Disparities in Substance Misuse: The Role of Childhood Abuse and Intimate Partner Violence Among Patients in Care at an Urban Community Health Center. Substance Use & Misuse, 48(3), 274–289. https://doi.org/10.3109/10826084.2012.755702
- Ristock J. L. (2003). Exploring dynamics of abusive lesbian relationships: preliminary analysis of a multi-site, qualitative study. Am. J. Community Psychol. 31 3–4. 10.1023/A:1023971006882
- Ristock J. L., Timbang N. (2005). Relationship violence in lesbian/gay/bisexual/transgender/queer (LGBTQ) communities. Retrieved January 29, 2019, from https://pdfs.semanticscholar.org/23b6/1c0642d6b09fe881fc4c3e465e59905dccc6.pdf
- Renzetti C. M. (1988). Violence in lesbian relationships: A preliminary analysis of causal factors. Journal of Interpersonal Violence, 3, 381–399. doi:10.1177/088626088003004003
- Same-sex Couple Data & Demographics – The Williams Institute. (n.d.). Retrieved January 29, 2019, from https://williamsinstitute.law.ucla.edu/visualization/lgbt-stats/?topic=SS&area=22&compare=total#comparison
- Simpson, E. K., & Helfrich, C. A. (2007). Lesbian survivors of intimate partner violence: Provider perspectives on barriers to accessing services. Journal of Gay & Lesbian Social Services, 18(2), 39.
- Smith, S.G., Zhang, X., Basile, K.C., Merrick, M.T., Wang, J., Kresnow, M., Chen, J. (2018). The National Intimate Partner and Sexual Violence Survey (NISVS): 2015 Data Brief – Updated Release. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Retrieved January 30, 2019, from https://www.cdc.gov/violenceprevention/pdf/2015data-brief508.pdf
- Stephenson, R., & Finneran, C. (2017). Receipt and Perpetration of Intimate Partner Violence and Condomless Anal Intercourse among gay and bisexual men in Atlanta. AIDS and Behavior, 21(8), 2253–2260. https://doi.org/10.1007/s10461-017-1709-6
- Stuart, G. L., McGeary, J., Shorey, R. C., Knopik, V., Beaucage, K., & Temple, J. R. (2014). Genetic Associations with Intimate Partner Violence in a Sample of Hazardous Drinking Men in Batterer Intervention Programs. Violence against Women, 20(4), 385–400. https://doi.org/10.1177/1077801214528587
- The National Domestic Violence Hotline: LGBTQ Abuse, Relationship Violence. (2019, January 30). Retrieved February 3, 2019, from https://www.thehotline.org/is-this-abuse/lgbtabuse/
- Walters, M. L., Chen, J., & Breiding, M. J. (2013). The National Intimate Partner and Sexual Violence Survey: 2010 Findings on Victimization by Sexual Orientation: (541272013-001)[Data set]. American Psychological Association. https://doi.org/10.1037/e541272013-001
- World Health Organization. (2012). Understanding and addressing violence against women (p. 1). Retrieved from https://apps.who.int/iris/bitstream/handle/10665/77432/WHO_RHR_12.36_eng.pdf;jsessionid=7D2607E06D69E9E25C40E31540F68CA0?sequence=1
Figures
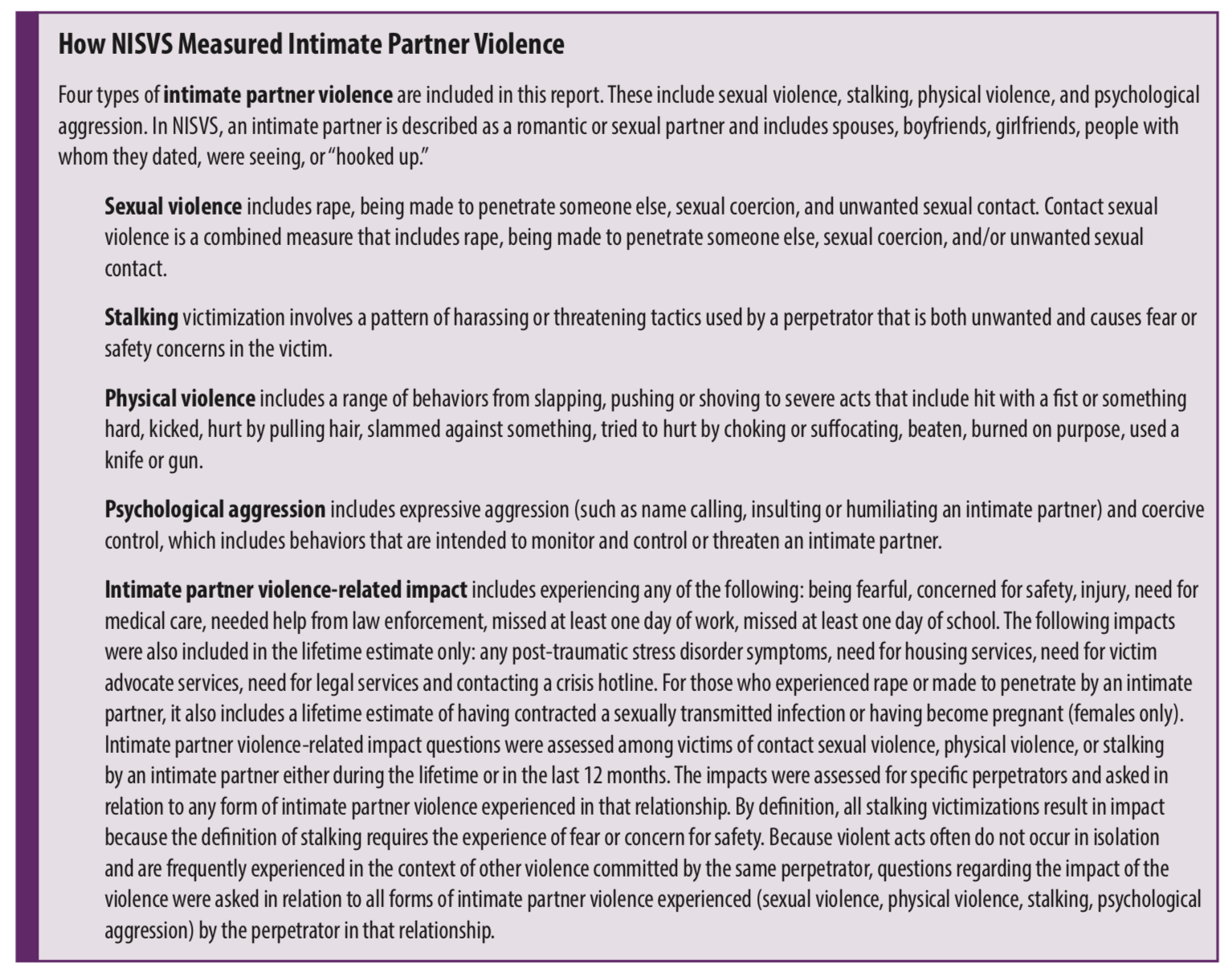
Figure 1. Definition of Intimate Partner Violence (Smith, et al, 2018)
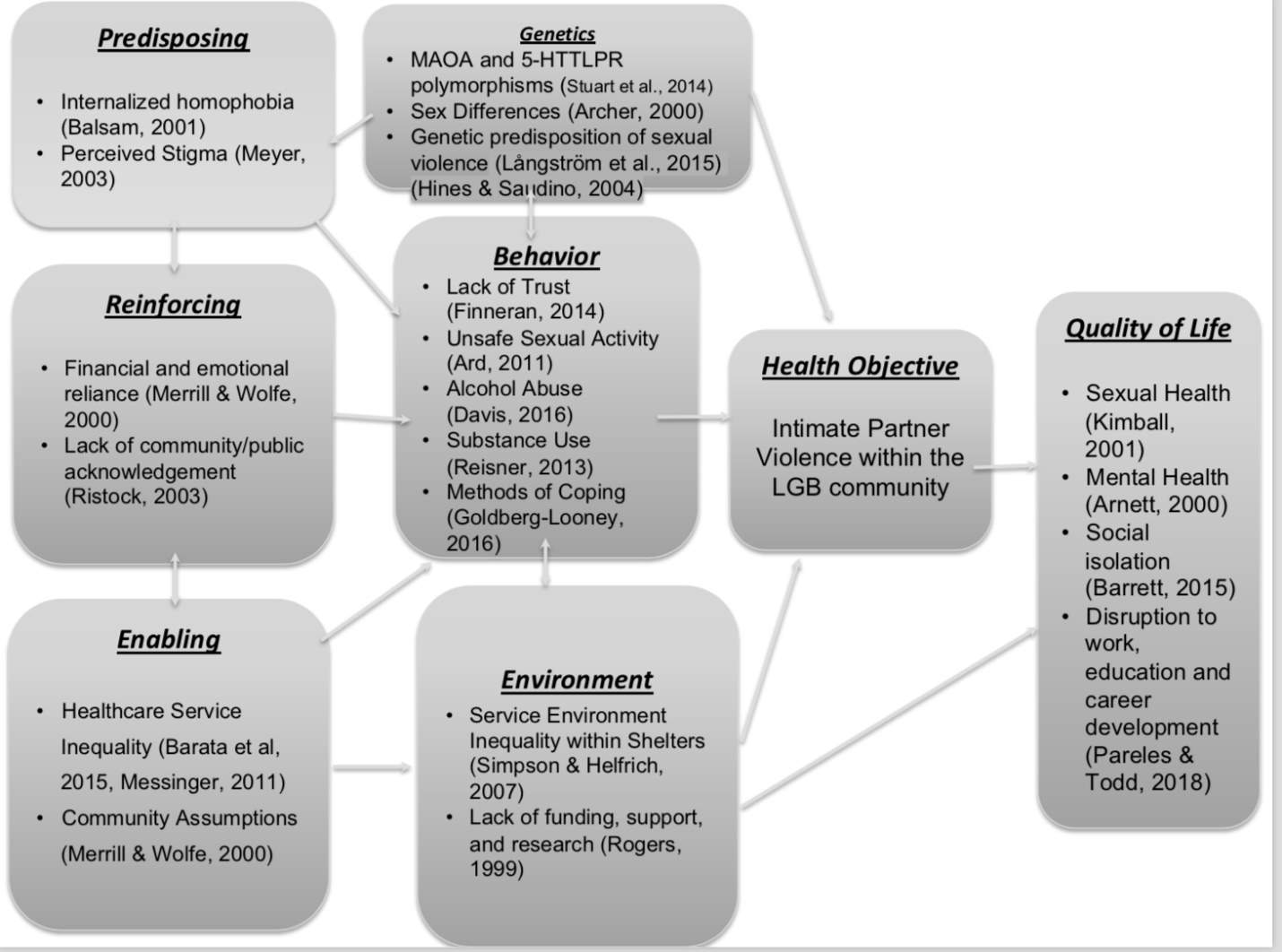
Figure 2. Conceptual Model of IPV in LGB Community
Cite This Work
To export a reference to this article please select a referencing style below: