
6-weeks Physical Rehabilitation Protocol for Anterior Glenohumeral Subluxation in Athletes
Abstract:
Background: Anterior shoulder dislocations and subluxations are common in young athletes. The mechanism for the first or primary shoulder dislocation may involve a collision or a fall typically with the arm in an abducted and externally rotated position. Contact sports, such as rugby and ice hockey, provide frequent opportunities for this injury to occur. Shoulder dislocations can occur after much less trauma in patients with previous dislocations. Despite a period of immobilization and rehabilitation following traumatic dislocations, recurrent instability often results and can lead to significant disability. To minimize the need for surgical intervention, effective physical rehabilitation programs are needed.
Purpose: The aim of this study was to design a physical rehabilitation program using elastic band and resistive exercise to improve joint strength and range of motion in individuals diagnosed with a first-time shoulder dislocation.
Method: Twelve physically active males with a first-time acute shoulder dislocation were asked to volunteer. Participants began a physical rehabilitation program two weeks after the shoulder dislocation, which was confirmed by a referring physician. The rehabilitation program was 6 weeks in duration and required the participants to engage in progressive resistive loads/duration using elastic bands and weights five days per week. Pretest and posttest measures included shoulder strength and range of motion. All outcome measures were compared between the injured and uninjured shoulder, which served as the control condition in this study.
Get Help With Your Essay
If you need assistance with writing your essay, our professional essay writing service is here to help!
Results: There were statistically significant differences between the injured and uninjured shoulder for measures of strength and range of motion during pretests (p < 0.01) but not posttests (p < 0.53). The magnitudes of differences during pretests were typically greater than 50%. Finally, there were no differences between shoulders in regards to the volume measure suggesting that any changes in muscle atrophy or swelling were not detected.
Conclusions: The physical rehabilitation program proposed in this study was effective at improving strength and range of motion in the injured shoulder as evidenced by the similarity in posttest values between the injured and uninjured shoulder. These results are encouraging and suggest the physical rehabilitation program proposed in this study may help reduce the need for surgical intervention in healthy young males who experience a primary shoulder dislocation.
Introduction:
The shoulder is the most frequently dislocated joint in the human body, anterior dislocation being the most common injuries in our daily life, especially for young people (Rumian, et al., 2011; Liu, et al., 2014). It was estimated that the incidence rate of shoulder dislocation as 23.9 per 100,000 persons a year (Owens, et al., 2009). Anterior shoulder dislocations and subluxations are common injuries in young athletes (Kaplan, et al., 2005; Malhotra, et al., 2012). The disparity between the large humeral head and the small glenoid cavity gives the joint the ability to be injured (Brukner, 2012; Brandt, et al., 2013) Moreover, the anteriorly dislocated humeral head causes a labrum tear of the anterior and inferior labrum, a Bankart injury (UG, et al., 2014; Porcellini, et al., 2009), and a typical impression fracture (Hovelius, et al., 2008; Kim, et al., 2003). The mechanism of the first dislocations occurs after a forceful direct trauma or a fall typically with the arm in an abducted and externally rotated or outstretched arm (Owens, et al., 2010; Rolf, 2007). Thus, in the majority of cases, the arm is abducted and the shoulder is externally rotated (Hardy, et al., 2010; Patel, et al., 2010). This is common in rugby, hockey, Handball, Football, riding, and cycling. In patients with lax shoulders or previous dislocations, dislocation can occur after much less trauma (Badr & Gaballah, 2015; Kelly & Terry, 2001; Brooks, et al., 2005). Recently, the most common management of treatment for primary anterior glenohumeral instability is nonoperative management (Gibson, et al., 2004; Zacchilli & Owens , 2010) Rehabilitation and prevention of this injury were worthwhile of research because negligence of rehabilitation the first-time dislocation shoulder may lead to recurrent instability of the glenohumeral joint (Rumian, et al., 2011; Provencher, et al., 2010). Furthermore, there is a body of reports suggesting that younger athletes generally and contact sports particularly most affected with the instability risk after a primary anterior shoulder dislocation. (Zacchilli & Owens , 2010; Handoll, et al., 2006). This risk of the recurrence dislocation reported in young athletes with first-time anterior dislocation as height as 90-95% (Gibson, et al., 2016). However, the athletes with anterior shoulder dislocation which returning to activities with in season after lack rehabilitation have demonstrated high rates of recurrent dislocation from 37% to 90%. (Watson, et al., 2016; Castagna, et al., 2007). The goal of the primary rehabilitation for the acute anterior shoulder is to prevent long-term instability for the shoulder joint (Leroux, et al., 2014). However, patients with recurrent shoulder instability often need to surgical intervention or arthroscopic treatment. (Malhotra, et al., 2012; Provencher, et al., 2010; Porcellini, et al., 2009).
Indeed, several modalities used conservative treatment for the acute dislocation shoulder (Liu, et al., 2014; Yamamoto, et al., 2010; Liavaag, et al., 2011) and injections (Nagata, et al., 2016). Some approaches have been conducted physical rehabilitation programs for first-time dislocation shoulder (Gibson, et al., 2004; Karatsolis & Athanasopoulos, 2006; Salamh & Speer, 2013). Other used the elastic resistance exercise which became one of the popular tools in physical rehabilitation. (Andersen, et al., 2010; Camci, et al., 2013; Brandt, et al., 2013) The major reason to use the elastic band that they have demonstrated excellent validity and reliability with shoulder muscle testing (Andersen, et al., 2016). Ultimately, the aim of this study was to design a physical rehabilitation program using an elastic band and resistive exercise to improve joint strength in individuals diagnosed with a first-time shoulder dislocation.
Method:
Subjects
Physically active males who presented at the Mansoura university hospitals and the teaching hospital in Damietta, Egypt with acute anterior dislocation shoulder injury between September 2012 and February 2015 were randomly recruited as research participants. The magnetic resonance imaging (MRI) were conducted to determine the injury grade for 17 athletes. We excluded patients with recurrent dislocation shoulder or had a history of injury in the same joint. Twelve physically active males (age 18.6 ± 1.32y, mass 74.48±3.22 Kg, height 178.4±3.21 cm and competitive experience 9.6±2.67 y) with a first-time acute shoulder dislocation were considered as research participants. The participants began a physical rehabilitation program two weeks after the shoulder dislocation, which was confirmed by a referring physician.
Rehabilitation Program
The external and internal rotation exercises have been chosen for the first stage which aimed to control the pain and inflammation caused by the dislocation and included seventeen flexibility and isotonic strength exercise with 12-15 1RM intensity were performed for the scapulothoracic muscles particularly, the rotator cuff muscles. (Figure 1).

Fig 1. First rehabilitation stage exersices examples

Fig. 2. Second rehabilitation exercises examples.
The second stage aimed to restore higher level of muscle strength. The intensity of exercises was five sets with 8-10 1RM, was tested according to the healthy arm. Thirty-two exercises in particular, Deltoid M., Trapezius M. and serratus anterior M. exercises in this stage were performed widely in the horizontal and diagonal axes. Moreover, the exercises were chosen to enhance the range of motion (ROM) and muscles strength between 90-150° vertically, horizontally, and diagonally (Figure 2). The third stage, after the twenty rehabilitation sessions. The endurance, peromitric, and strength exercises were consisted of five sets of 8-10 repetitions using variable resistance: one at 75% of the 10 RM, and two at 95% of the 8 RM. 27 extremity weights rehabilitation exercises performed to reach 190 - 200° ROM and the equally health arms strength as well. (Figure 5,6). The Thera-Band resistance bands exercises were hired during the six weeks especially the four colors (red, blue, black, silver, gold). The red and blue bands were used in the first stage and the black and silver used in second stage, addition, the gold has been performed in the third stage. Furthermore, all the exercises performed by stretching the band between 75 - 100 %. knowing that, the weight of stretching in Thera-Band between 75-100% is (red 3.3-3.9kg, blue 5.9-7.1kg, black 8.1-9.7, silver 11.1-13.2kg, and gold 18.1-21.6kg). (BiÇer, et al., 2015;Andersen, et al., 2010)

Fig. 3. Third rehabilitation exercises examples.
Statistics analyze:
The paired t-test was used to compare the collected data before performing the exercise protocol (Pre-test) and those which obtained after 6-weeks physical rehabilitation period (Post-test). Whether the differences between the samples were significant at p < 0.05 level and p < 0.01. All the analyses were performed by using SPSS 19 software for Windows 7 (SPSS Inc. Chicago, IL, USA). Additionally, all values within the text and table are observed as standard deviation and mean (mean ± SD).
Measurements:
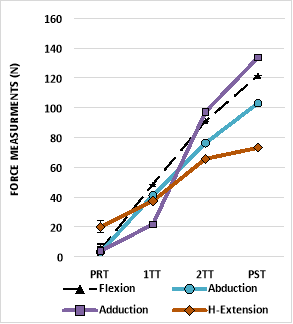
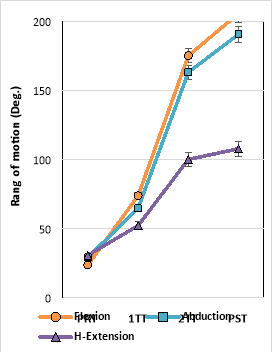
The rehabilitation program was comprised four testing sessions. The Pre-test (PRT) section was conducted after two weeks of the injury and before the beginning of the rehabilitation program. after two rehabilitative weeks, the second week tracking test (SWT) was realized. while the Fourth week tracking test was realized after the fourth rehabilitative week (FWT). Moreover, after a resting of 6 weeks, the Post-test was conducted in the Faculty of Sports Education, Damietta University, Egypt. Additionally, all the injured athletes were right handed injured and in each testing test, the healthy arms measurements were recorded. Continuously, the test results for the injured arm had been compared with the healthy arm for each person. Before reporting the force measurement all the participants were informed with the test procedures for both arms. Four basics Isotonic force measurements were reported by Isometric Dynamometer device (Biodex Isokinetic Dynamometer). These force measurements were conducted for muscles around shoulder girdle in the 90 Deg. vertically and horizontally. The force variables were flexion force (F.F), adduction force (AD.F), Abduction force (AB.F), and hyper extension force (HB.F). Whilst, the participants were asked to perform the maximum flexibility for the shoulder joint without feeling pain. Addition, the range of motion variables were obtained by Goniometer for flexion range of motion (F.ROM), abduction (AB.ROM), and hyper extension (HB.ROM).
Results:
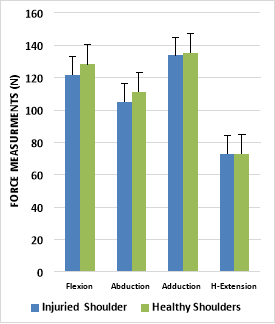
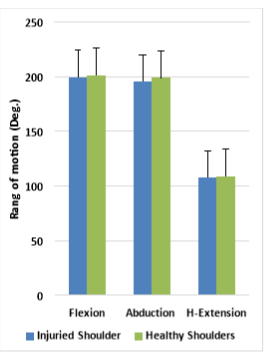
The test results (i.e., strength and range of motion) shown that there were statistically significant differences between the injured and uninjured shoulder (p > 0.01) prior the rehabilitation procedure. After six weeks of physical rehabilitation, the test results shown considerable improvement of more than 50%. As obviously seen from table 1, the deference between the pre-testes and post- testes of force were, flexion force 4.41 ±4.01N vs 121.5±12.4 N, abduction force 2.94±2.74 N vs 103.1± 9.8 N, Adduction 3.84±0.34 vs 133.7±9.26,Hyper-Extension 20.01±7.64 N vs 69.1±8.92 N. On the other hand, the range of motion of pre-testes and post-test were, Flexion 23.8±4.02â° vs 199.5±0.24â°, Abduction was 29.3±3.62â° vs 195.5±2.13â°, Hyper-extension 30.8±5.81â° vs. 108.5±5.72. Furthermore, the conducted post tests shown that there were no significant differences (p < 0.53) between the injured and uninjured shoulders. In addition, the participants' injured shoulder showed great improvement after the rehabilitation. In addition to the post tests of the injured and uninjured shoulders were, Flexion force 121.5±12.44 N vs 128.2±10.4 N with 94% enhancement, abduction force 103.1± 9.81 N vs 110.9±8.32N with 93% enhancement, adduction 133.7±9.26 vs 135.2±5.33 with enhancement 99%, Hyper-extension 69.1±8.92 N vs 72.71±5.42 N with 95% enhancement. In contrast, F.ROM 199.5±0.24â° vs201.3±1.25â° with 99% enhancement, AB.ROM 195.5±2.13â° vs 198.9±1.06â° with 98.3% enhancement, and HE.ROM 107.8±6.12â° vs 108.5±5.72â° with 99.4% enhancement. Finally, the rehabilitation did not induce any side effects; muscle atrophy changes and swells were not detected.
Table 1. Improvement of the measurement among the rehabilitation stages.
|
Improvment |
Healthy Shoulders |
Post-Test |
FWT |
SWT |
Pre- Test |
Unit |
Variables |
|
|
94 % |
128.2±10.4 |
121.5±12.44 |
91.04±8.13 |
48.7±4.31 |
4.41 ±4.01 |
N |
Flexion |
Force |
|
93% |
110.9±8.32 |
105.1±9.81 |
76.2±10.41 |
41.3±5.92 |
2.94±2.74 |
N |
Abduction |
|
|
99% |
135.2±5.33 |
133.7±9.26 |
97.12±7.22 |
21.7±2.17 |
3.84±0.34 |
N |
Adduction |
|
|
95% |
72.71±5.42 |
73.1±8.92 |
65.7±4.51 |
37.04±4.21 |
20.01±7.64 |
N |
H-Extension |
|
|
99.1% |
201.3±1.25 |
199.5±0.24 |
168±7.48 |
73.8±8.32 |
23.8±4.02 |
Deg |
Flexion |
ROM |
|
98.3% |
198.9±1.06 |
195.5±2.13 |
163±6.94 |
64.7±8.81 |
29.3±3.62 |
Deg |
Abduction |
|
|
99.4% |
108.5±5.72 |
107.8±6.12 |
100±2.2 |
52.2±13.2 |
30.8±5.81 |
Deg |
H-Extension |
|
Discussion:
The current study aimed to design a rehabilitation program passed on the elastic and weights exercises. Over the past decades, we have seen a huge boost in the rehabilitation of shoulder dislocation injuries. These injuries because of the anatomical structure of the glenohumeral joint which allow to wide movement of the joint. Therefore, derives its extensive movement at the expense of its consistency and coherence. More than 50% of acute anterior dislocations can reoccur, especially in young athletes. The aim of the physical rehabilitation is avoiding the recurrent dislocation and using an elastic band and resistive exercise to improve joint strength in individuals diagnosed with a first-time shoulder dislocation.
Find Out How UKEssays.com Can Help You!
Our academic experts are ready and waiting to assist with any writing project you may have. From simple essay plans, through to full dissertations, you can guarantee we have a service perfectly matched to your needs.
View our academic writing services
The current study results shown that, there were weakness of the shoulder muscles in the pre-test measurements of Flexion, adduction, abduction force as a result of ache, swelling, and inflammation. Nevertheless, the hyperextension motion measurements were reported better than the other measurement in the pretest. The mechanism of the anterior dislocation occurred forwardly and downward. Out of the ordinary, that has affected adversely on the forward movement of the arm. (Turkel, et al., 1981)
The return to activity after 2-3 weeks is available for athletes with a high risk of recurrence dislocation. which expected to arthroscopic remain and return to activity after 6-month surgical stabilization (Watson, et al., 2016). Many factors have been related to rehabilitate shoulder dislocation. Thus, the current study has been assumed that 6 weeks' elastic resistant with weight exercise had great benefit for the shoulder muscles especially, the rotator cuff muscles. Recently, the popularity of elastic bands has increased because of their low prices, flexibility, adaptability, versatility, and simplicity. (Andersen, et al., 2010) (Jakobsena, et al., 2013). The incorporation between nautilus machine and the elastic bands exercises have been used to promote joint range of motion and muscles strength in training and rehabilitation purposes as well. thus, the elastic resistant exercise has been improved the influences of the strength-shorting cycle. Addition to, it has been used as technique to produce the speed eccentric contraction. (Stevenson, et al., 2010).
It is obviously seen in table 1. and Figure 2, 3. there are a considerable significant different between the pretests and the posttests of the injured shoulders. Addition, it is seeming to be similar with the healthy shoulder after the 6wks. physical rehabilitation program. The same resulted reported in previous study conducted on young volley ball players and have improved their muscle power, muscle strength and ball speed. (Mascarin, et al., 2016). Nevertheless, the elastic resistant and free weight exercise improve the dynamic stabilization and joint stability. (Andersen, et al., 2010) (Camci, et al., 2013). Addition, the exercise rehabilitation program for the unstable shoulder must include a joint position sensibility and dynamic stabilization to supporting the functional stability of the shoulder joint. The dynamic stabilization is promoted the co-activation of the force couples about the glenohumeral joint to exceptional position of the humerus hear in the center of glenoid. (Naughton, et al., 2005). Previous studies have demonstrated same levels of muscle activation for using elastic resistance compared with free weights display similar or even greater levels of muscle activity for some muscles during an exercise. (Camci, et al., 2013) (Andersen, et al., 2010). In contrast, used parallel with free weight (Aboodardaa, et al., 2013). Other studies have shown high levels of muscles activation compared with weight machine (Brandt, et al., 2013). But all the modalities recommended to use the elastic band with the weights. Moreover, using elastic band with weights appear to be equally in muscle activity as traditional using isoinertial resistance (Jakobsena, et al., 2013). Finally, The physical rehabilitation program proposed in this study was effective at improving strength and range of motion in the injured shoulder as evidenced by the similarity in posttest values between the injured and uninjured shoulder. These results are encouraging and suggest the physical rehabilitation program proposed in this study may help reduce the need for surgical intervention in healthy young males who experience a primary shoulder dislocation.
Aboodardaa, S. J. et al., 2013. Resultant muscle torque and electromyographic activity during high intensity elastic resistance and free weight exercises. European Journal of Sport Science, 13(2), pp. 155-163.
Andersen, L. et al., 2010. Muscle Activation and Perceived Loading During Rehabilitation Exercises: Comparison of Dumbbells and Elastic Resistance. Physical Therapy, 90(4), pp. 538-549.
Andersen, L., Vinstrup, J., Jakobsen, M. & Sundstru, E., 2016. Validity and reliability of elastic resistance bands for measuring shoulder muscle strength. Scand J Med Sci Sports., Volume May.
Badr, M. & Gaballah, A., 2015. Common Injuries among Male Field Hockey Players According to Playing Positions.. Journal of Applied Sports Science, 5(1), pp. 19-26.
BiÇer, M. et al., 2015. Effect of Strength Training Program with Elastic Band on Strength Parameters. Biology of Exercise , 11(2), pp. 111-122.
Brandt, M. et al., 2013. Perceived loading and muscle activity during hip strengthening exercises: comparison of elastic resistance and machine exercises.. Int J Sports Phys Ther, 8(6), pp. 811-819.
Brooks, J., Fuller, C., Kemp, S. & Reddin, . D., 2005. Epidemiology of injuries in English professional rugby union: part 2 training injuries. British Journal of Sports Medicine, Volume 39, pp. 767-775.
Brukner, P., 2012. Clinical sports medicine. 4 ed. Australia: McGraw-Hill Publishing.
Camci, E. et al., 2013. Scapular Kinematics During Shoulder Elevation Performed With and Without Elastic Resistance in Men Without Shoulder Pathologies. Journal of Orthopaedic & Sports Physical Therapy , 43(10), pp. 735-743.
Castagna, A., Nordenson, U., Garofalo, R. & Karlsson, J., 2007. Minor shoulder instability. The Journal of Arthroscopic & Related Surgery, Volume 23, pp. 211-215.
Gibson, K. et al., 2004. The effectiveness of rehabilitation for nonoperative management of shoulder instability: a systematic review. Journal of Hand Therapy, 17(2), pp. 229-242.
Handoll, H., Hanchard, N., Goodchild, L. & Feary, J., 2006. Conservative management following closed reduction of traumatic anterior dislocation of the shoulder.. Cochrane Database Syst Rev., 25(1), p. CD004962.
Hardy, M., Summers, D., Edwards, J. & Munro, N., 2010. The BMA guide to sports injuries, Dorling Kindersley Puplishing, UK, 2010.. London, UK: Dorling Kindersley Puplishing.
Hovelius, L. et al., 2008. Nonoperative treatment of primary anterior shoulder dislocation in patients forty years of age and younger. A prospective twenty-five-year follow-up. J Bone Joint Surg, Volume 90, pp. 945-952.
Jakobsena, M. et al., 2013. Muscle activity during leg strengthening exercise using free weights and elastic resistance: Effects of ballistic vs controlled contractions. Human Movement Science , 32(1), pp. 65-78.
Kaplan, L. et al., 2005. Prevalence and variance of shoulder injuries in elite collegiate football players. 2005;33:1142-6.. Am J Sports Med. , Volume 33, pp. 1142-1146.
Karatsolis, K. & Athanasopoulos, S., 2006. The role of exercise in the conservative treatment of the anterior shoulder dislocation. Journal of Bodywork and Movement Therapies, Volume 10, pp. 211-219.
Kelly, L. & Terry, G., 2001. Team Handball: Shoulder Injuries, Rehabilitation, and Training. Sports Medicine & Arthroscopy Review:, 9(2), pp. 115-123.
Kim , S. et al., 2003. Accelerated rehabilitation after arthroscopic Bankart repair for selected cases: a prospective randomized clinical study.. Arthroscopy, 19(7), pp. 722-731.
Leroux, T. et al., 2014. Epidemiology of Primary Anterior Shoulder Dislocation Requiring Closed Reduction in Ontario, Canada. The American Journal of Sports Medicine, 42(2), pp. 442-450.
Liavaag, S. et al., 2011. Immobilization in external rotation after primary shoulder dislocation did not reduce the risk of recurrence: a randomized controlled trial.. J Bone Joint Surg Am, 93(10), pp. 897--904.
Liu, A. et al., 2014. The external rotation immobilisation does not reduce recurrence rates or improve quality of life after primary anterior shoulder dislocation: A systematic review and meta-analysis.. Injury, Int. J. Care Injured, Volume 45, pp. 1842-147.
Malhotra, A., Freudmann, M. S. & Hay, S. M., 2012. Management of traumatic anterior shoulder dislocation in the 17- to 25-year age group: a dramatic evolution of practice. J Shoulder Elbow Surg, Volume 21, pp. 545-553.
Mascarin, N., De Lira, C., Vancini, R. & Andrade, M., 2016. Strength Training Using Elastic Band Improves Muscle Power and Throwing Performance in Young Female Handball Players. Journal of sport rehabilitation, Volume 24, pp. 1-25..
Nagata, H., Thomas, W. & Woods, D., 2016. The management of secondary frozen shoulder after anterior shoulder dislocation - The results of manipulation under anaesthesia and injection. journal of orthopaedics, Volume 13, pp. 100-105.
Naughton, J., Adams, R. & Maher, C., 2005. Upper-body wobbleboard training effects on the post-dislocation shoulder. Physical Therapy in Sport, Volume 6, pp. 31-37.
Owens, B. et al., 2009. Incidence of Glenohumeral Instability in Collegiate Athletics.. 37(9), pp. 1750-1754.
Owens, B. et al., 2010. Pathoanatomy of First-Time, Traumatic, Anterior Glenohumeral Subluxation Events. The Journal of Bone and Joint Surgery, 92(7), pp. 1605-1611.
Patel, D. R., Greydanus, D. E. & Bak, R. J., 2010. Pediatric Practice Sports Medicine. New York, USA: McGraw-Hill.
Porcellini, G. et al., 2009. Predisposing Factors for Recurrent Shoulder Dislocation After Arthroscopic Treatment. J Bone Joint Surg Am, 91(11), pp. 2537-2542.
Provencher, M. T. et al., 2010. Recurrent Shoulder Instability: Current Concepts for Evaluation and Management of Glenoid Bone Loss. J Bone Joint Surg Am, 92(2), pp. 133-151.
Rockwood, C. A., 2008. The Shoulder. 4 ed. s.l.:Elsevier, Health Science Publisher.
Rolf, C., 2007. Sports Injuries Hand Book, Diagnosis and Management. London: A & C Black Publishers.
Rumian, A., Coffey, D., Fogerty, S. & Hackney, R., 2011. Acute first-time shoulder dislocation. Orthopaedics and Trauma, 25(5), pp. 363-368.
Salamh, P. A. & Speer, K. P., 2013. Post-Rehabilitation Exercise Considerations Following Total Shoulder Arthroplasty. Strength & Conditioning Journal, 35(4), pp. 56-63.
Stevenson, M. et al., 2010. Acute Effects of Elastic Bands During the Free-weight Barbell Back Squat Exercise on Velocity, Power, and Force Production. Journal of Strength & Conditioning Research, 24(11), pp. 2944-2954.
Turkel, S., Panio, M., Marshall, J. & Girgis, F., 1981. Stabilizing mechanisms preventing anterior dislocation of the glenohumeral joint.. J Bone Joint Surg Am, 63(8), pp. 1208-1217.
UG, L. et al., 2014. Management of primary acute anterior shoulder dislocation: systematic review and quantitative synthesis of the literature.. Arthroscopy, 30(4), pp. 506-522.
Yamamoto, N., Sano, H. & Itoi, E., 2010. Conservative treatment of first-time shoulder dislocation with the arm in external rotation. J Shoulder Elbow Surg, Volume 19, pp. 98-103.
Zacchilli, M. & Owens , B., 2010. Epidemiology of shoulder dislocations presenting to emergency departments in the United States. J Bone Joint Surg Am , Volume 92, p. 542-549.
Anterior shoulder dislocation
Cite This Work
To export a reference to this article please select a referencing style below: