
Why do we need to embed ourselves in practice? A review of the literature considering the need to experience mindfulness practice and have a regular practice to teach MBCT/MBSR
Introduction:
Mindfulness Definitions:
What is mindfulness? This has become in recent years an ever more diverse and contentious question[DD2] (Shapiro 2009, Monteiro et al 2015). With The huge expansion of interest in mindfulness and mindfulness based interventions[DD3] (MBIs) such as [DD4]Mindfulness Based Cognitive Therapy and Mindfulness Based Stress Reduction (MBCT/MBSR) it seems important to offer some definitions. The history of mindfulness is rich and varied. Mindfulness skills have been applied in many different cultures in human life for thousands of years. The contemplative and meditative knowledge suggested have been found in the background of different religious backgrounds, Hinduism, Buddhism, Islam, and Christianity, and in different cultures, India, Asia, Europe and America. There is a history in the far past, in the middle Ages and in modern times.
Mindfulness background commonly known and taught within the majority of mindfulness based courses in the UK sits within a Buddhist tradition. ÅšÄntideva (2004) offers an analogy from Buddhist literature about mindfulness:
“Rutting elephants roaming wild do not cause as much devastation in this world as the roaming elephant, the mind, let free, creates… But if the roaming elephant, the mind, is tethered on every side by the cord of mindfulness, every danger subsides, complete prosperity ensues. “
ÅšÄntideva (BodhicaryÄvatÄra, 5, 2-3)
Traditional and modern mindfulness have appreciated a more common exchange of knowledge and practice applications than often is originally recognised. Monteiro et al (2015[DD5]) discuss the concept that there is a common thread within traditional and more contemporary mindfulness practices to alleviate suffering by being present with our experience with kindness. That we can rein the roaming mind somehow by practice of being with our experience compassionately. Modern Buddhism and more recent MBIs such as MBCT/MBSR seek to address subjects such as living with chronic illness (Bernhard 2010), happiness (Ricard 2008), work (Salzburg 2013), and other topics traditionally considered the focus of Western psychology[DD6] by drawing on these traditional practices.
Jon Kabat-Zinn, although he argues for the setting [DD7]of mindfulness and MBSR very much to sitting within a Buddhist framework, developed one of the most common definitions of mindfulness offered in more modern or secular texts:
“The practice of paying attention in a particular way: on purpose, in the present moment, and non – judgmentally”
(Kabat-Zinn, 1994: p. 4).
Bishop et al (2004) from a much more secular stance, attempt to operationally define mindfulness offer this.
“..We see mindfulness as a process of regulating attention in order to bring a quality of non-elaborative awareness to current experience and a quality of relating to one’s experience within an orientation of curiosity, experiential openness, and acceptance. We further see mindfulness as a process of gaining insight into the nature of one’s mind and the adoption of a de-centred perspective…on thoughts and feelings so that they can be experienced in terms of their subjectivity (versus their necessary validity) and transient nature (versus their permanence).”
(Bishop et al, 2004: p. 234).
Shapiro and Carlson (2009) offer a clear deï¬nition of mindfulness, carefully delineating between mindful awareness (big M mindfulness) and mindful practice (little m mindfulness). They offer a model of mindfulness with three core elements intention, attention, and attitude. Intention being the way one approaches practice, attention being at the heart of our practice, the quality of how one pays attention, and attitude being the non-judgmental open stance adopted.
Get Help With Your Essay
If you need assistance with writing your essay, our professional essay writing service is here to help!
It is of noted that all of these definitions of mindfulness are suggesting a kind, of as Shapiro and Carlson note in their model (2009) attitudinal focus of the mind which is learnt, suggesting the development of this attitudinal stance as a ‘skill’, and perhaps ’embodiment’ (attitude and awareness) as a skill also to be learnt over time. According to Kabat-Zinn[DD8] (1990, in Shapiro 2009), the morals of being mindful ourselves [DD9]are implicit in MBIs. There is a sense also shared in traditional and contemporary MBIs of the learning of the attitudinal skills of mindfulness. The sense of ‘learning’ a way of relating to our more difficult experiences which is then able to be ’embodied and taught[DD10].
“Instructors are expected to take personal responsibility for behaving ethically in their personal and professional lives. Kabat-Zinn suggests that ethics are conveyed to patients through how instructors embody ethical behaviour in their own lives and in how they relate to patients. Ethics and mindfulness mutually support each other. One who is mindful will tend to act ethically[DD11].”
(Groves 2015, p.5)
Mindfulness Based Interventions (MBIs)
MBSR and MBCT
Jon Kabat-Zinn and his colleagues[DD12], who developed an eight-week course in mindfulness for people with chronic health conditions at the Massachusetts Medical School, USA[DD13], known as Mindfulness-Based Stress Reduction (MBSR) (Kabat-Zinn 1982.). This 8 week MBSR course format has become widely used and well researched and is widely around the world, for a variety of different health conditions[DD14]. (Kabat-Zinn 1998, 2005)
“MBSR spans a confluence of epistemologies and practices from two very distinct and until recently, divergent lineages, both committed to empirical investigation, albeit utilizing very different methodologies: that of science, medicine, and psychology, on the one hand, and that of Buddhist meditative traditions and their teachings and practices, known collectively as the Dharma, on the other[DD15].”
Center for Mindfulness UMASS
There is a clear sense with MBSR of intention to interweave the Buddhist and medical/psychological schools of thought to provide an intervention, which is taught by those considered skilled.
Teasdale et al (2000, 2010, and 2012) adapted the MBSR course for people who had suffered from depression, as a way to prevent relapse. They called their course Mindfulness-Based Cognitive Therapy (MBCT). Teasdale et al (2003) [DD16]undertook randomized controlled trials (RCTs) with the manualised MBCT created produce data on its efficacy[DD17]. They found that MBCT particularly benefits patients with major depressive disorder (MDD) episodes. Two RCTs (Ma & Teasdale, 2004; Teasdale et al., 2000), both of which stratified participants prior to randomization by number of episodes (2 versus 3 or more), found that MBCT lowered risk of relapse in case of three or more MDD episodes
MBCT is a much more overtly secular course with little reference to Buddhist background in the manual. It still though contains some guidance about the person of the teacher, and within the RCT the standard for those running the groups was that they had been trained and were considered ‘competent’. A criticism of this RCT [DD18]may be that the ‘competence’ of those running the groups is not well defined, and might be considered a variable within the study.[DD19]
Structurally, MBCT and MBSR have many factors in common: Programs that are held weekly for 8-12 weeks engage in dialogues between teacher and participant that explore the experiential aspects of practice (called an inquiry) and delivery to groups of eight or larger. Some practices are similar: meditations such as the body scan, awareness of breath, loving-kindness, and mindful movements. They may differ in the details of the curriculum that are mandated by the intent of the program (relapse prevention, behavioural activation/inhibition, or self-discovery). The commonality of this structure has allowed for a large number of investigations into the efficacies of treatment approaches and explorations of the way in which mindfulness components function together[DD20]. This research into the mechanisms and effectiveness of MBIs has grown exponentially in the last 5 years (Black 2014[DD21], Teasdale et al 2000, 1992.)
Mindfulness is used in induvial therapy also. Here it may sit within a therapeutic framework such as Acceptance and Commitment Therapy (ACT), Dialectical Behavioural Therapy (DBT) or Compassion Focused Therapy (CFT) for example. There is also an expansion of Mindfulness Based Individual Therapy (MBIT). For the purposes of this literature review the use of mindfulness within induvial therapy has not been considered[DD22].
What is being embedded in our practice, how does it inform teaching?
“McCown et al (2010) discusses the skills of the MBCT/MBSR group facilitator, talking of the guidance of the group is being one of the key educational actions in the group. He also discusses what he calls ‘stewardship, homiletics and inquiry’. These skills are interconnected and each includes and influences the others. McCown discusses the three circles of experience (see fig 1) and suggests one must be skilled in knowing where one is, as well as where people in the group, or the groups as a whole are.




Fig 1. Representation of Philosophy and approach to teaching mindfulness: Adapted from McCown (2010)
As alluded to consistently throughout this introduction there is a thread from the origins and background of mindfulness, right to contemporary mindfulness which suggests that there is a skill and attitude to learn. McCown et al (2010) discusses the cultivation of present moment awareness, of being able to be with our experience with an attitude of compassion and non-judgement. Not unlike exercise the intention is to learn to tone up our ‘mindfulness muscle’ before showing others how to do this. It is posited that without that knowledge and learning of the skill by repeated practice of one’s own, one loses a great deal of this ’embodiment of the attitudes of present moment awareness and compassion [DD23]in the ‘holding’ and ‘stewardship’ of the group. This concept that McCown et al (2010) discuss suggest overtly ‘being grounded in our own instability’. (McCown 2010). They devote a chapter in their book to the person of the teacher which explicitly brings together many of the concepts discussed her. The integrity and authenticity of the teacher/instructor it is proposed is essential to be able to have effective stewardship of the group. To authentically undertake processes such as enquiry, and guiding practice[DD24] as a teacher, one needs to focus [DD25]on to really being with present moment experience authentically. McCown (2010) suggests that this repeated practice leads to a ‘spiritual maturity’ where as a teacher one can detach and have a sense of clarity and perspective, which can then be focused on cultivating the possibilities within the group.
The concept of embodiment is the representation or expression of something in a tangible or visible form. In terms of the mindfulness teacher this is suggesting that the person running the MBCT/MBSR group is more than just a facilitator but more holistically they represent a mindful stance in both verbal, but also in a more physical bodily way. Drummond (2006, cited in McCown et al 2010) discusses this important distinction as MBIs have been criticised for a cognitive bias, so this sense of embodiment, offering more than just. Words or explanation, but by being mindful in body and intent also brings much more to the experience.
Table 1. The essential (warp) and flexible (weft) ingredients of MBPs[DD26]
What is competency and fidelity?
There is a growing emergence of mindfulness based training [DD27]programmes (MBPs) both in the UK and further afield. It is interesting to note that these courses consider this idea of being embedded in a regular practice of one’s own an essential component of the learning to teach process. Crane et al (2016) offer a framework of ‘warp and weft’ which combines the formal training with the competency to understand what defines MBPs (see Table 1[DD28]). They argue that for the sustainable development of the field there is a need to articulate a definition of what an MBP is and what it is not[DD29]. (Crane et al 2016)
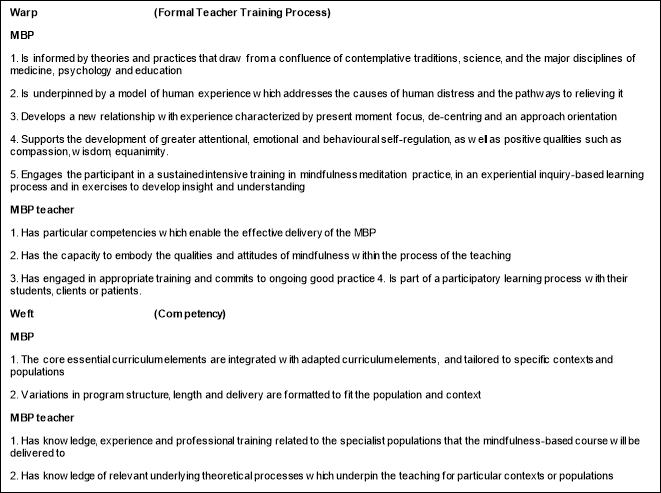
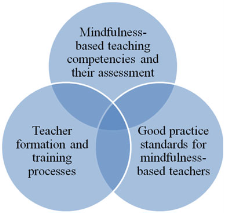
Fig. 2 working model of three interconnected aspects of quality and integrity in teaching mindfulness-based courses
(From Crane et al 2011 p.77)
Crane et al (2011) have the addition of ‘good practice’ in their earlier model of what offers ‘quality’ and ‘integrity’ to MBPs. In addition to being suggested in the ‘warp’ (essential) MBP competencies in this paper, Embodiment[DD30] is also a key concept suggested in good practice guidelines. The UK good practice guidelines (UK Mindfulness-Based Teacher Trainer Network, 2011) much more explicitly set out a standard of regular daily practice, engagement in retreats within their guidelines suggesting that this is an essential for good practice[DD31].
The NHS and moving towards MBIs in Clinical Settings in the UK
“The drive to train more MBSR professionals runs the risk of easily and inadvertently undermining the integrity, exactness and long-term commitment required for the formation and ongoing development of competent, well trained MBSR teachers “
(Center for Mindfulness in Medicine, Healthcare and Society, 2011, Conference Brochure[DD32])
In 2015 the Mindfulness All-Party Parliamentary Group (MAPPG) published the Mindful Nation UK (MNUK) report – the conclusion of a period of research and inquiry into the impacts of mindfulness training, including eight hearings in Parliament. This influential report looked at the scientific evidence for mindfulness and current best practice, and made some of the first concrete policy recommendations for UK government across four areas of public policy: criminal justice, healthcare, education and the workplace. The report concludes that while there is still much research to be done, mindfulness is already a promising innovation in the within the NHS with [DD33]an early but rapidly evolving evidence base. However, the report cautions that with the growing enthusiasm for mindfulness, many new providers of mindfulness training have emerged with very limited experience and qualification. Without an approved system of professional listings, companies have no objective way to evaluate the quality of potential providers. MAPPG (2015)
Find Out How UKEssays.com Can Help You!
Our academic experts are ready and waiting to assist with any writing project you may have. From simple essay plans, through to full dissertations, you can guarantee we have a service perfectly matched to your needs.
View our academic writing services
Crane et al. (2012a) cautioned that in the course of increasing opportunities for training people much more widely in mindfulness-based work, there is a risk that the integrity of the approach is watered down. This risk largely arises from the pressure between the need to teach mindfulness from the teacher’s personal experience of their own practice, embodied in the class, versus the pressure, which has now become marked within the NHS, to deliver NICE-approved interventions, such as MBCT, as widely and economically as possible. The literature discussed here on teaching mindfulness has repeatedly emphasises the centrality of embodiment to the teaching of mindfulness ( Kabat-Zinn 2005; Kabat-Zinn and Santorelli 2005; Segal et al. 2013). Crane et al. (2010) state that ‘the process of embodiment is a key feature of the teaching in a mindfulness-based class; it influences every aspect of the delivery of mindfulness-based stress reduction (MBSR)/MBCT, and thus, consequently, the training of the teachers who will be delivering it.’ However, this embodiment calls for a lasting commitment out of work time to the practice to allow the teacher to be embedded within their practice and embody the attitude, awareness and intention of mindfulness. A lack of understanding of this, put together with the economic pressures within the NHS, may lead to an approach in which mindfulness is just another method that can be added to the clinician’s currently existing range of skills and then taught, as if it were just another subject.
Rationale for this research
The introduction has sat out a clear history of a meditative, attitudinal state described above [DD34]within mindfulness which is learnt and then desirably embodied by those instructing/teaching. There is a rich history of this within Buddhist and other secular meditative traditions[DD35]. This ’embedding oneself in practice’ has been translated into more modern secular MBPs and is seen as a requirement of ‘competency’ by educational establishment and good practice guidelines published[DD36]. [DD37]The evidence provided for this concept though is often of the narrative variety from book sources or self-experience.
The NHS demand for MBIs specifically the NICE guidelines recommendation for MBCT/MBSR have created a demand for trained teachers/instructors that is significant (Crane et al 2010). There is also a variable output of courses within the NHS as staff are often although well intentioned offering MBCT/MBSR as teachers at different skill levels. Some argue that there is not a need for one’s own personal practice, and within the NHS the training and self-practice needed to reach the good practice guidelines is more often than not self-funded and in personal time. Now more than ever the case for the evidence to consider this rationale of ‘being within practice’ is salient and essential to offer a valid discourse on training and ongoing support for those offering MBIs[DD38].
Aim of research
The intention of this narrative literature review is to address the question of why we need to embed ourselves in practice to teach mindfulness based interventions (MBIs), specifically MCBT and MBSR. There is an intention to address a second question, is there good quality evidence to back up this idea. [DD39][YS40] There is a wealth of literature that talks about mindfulness[DD41], the stewardship of the groups when using an MBI, having fidelity and competency [DD42]as a teacher before we embark on our journey within teaching MBIs. (McCown 2010, Crane et al 2011, McCown 2013.) To begin to think about the question of what evidence there is to back up this concept it is useful first to define some key terms and concepts[DD43].
Research Questions??
Why do we need to embed ourselves in Practice?
What is the quality of the evidence surrounding this?
Methodology
The decision was made to undertake a narrative review. [DD44]Initially the idea of a systematic review was considered but the initial scoping seemed to indicate that there was not enough significant literature on this tropic to fulfil the requirements of a systematic review (SR), thus a narrative review (NR) was selected[DD45]. There is no consensus on the standard structure of an NR. The preferred format is the IMRAD (Introduction, Methods, Results, Discussion) which is what this review has worked to[DD46].
A recent report stated that NRs form the basis of medical literature synthesis, and their number per year in MEDLINE significantly surpassed that of SRs. (Bastian 2010) Although NRs and SRs differ in objectives, methods, and application areas, both may include several kinds of studies with different levels of evidence: randomised clinical trials, observational case-control or cohort studies, and case reports. Nevertheless, since NRs and SRs are written retrospectively, both are prone to bias.
Researchers use NR to achieve several objectives. To describe the current states of both art (i.e., practice) and science (i.e., research) in focused areas of inquiry; to add dimensions of insight or application that are not available in existing literature, and; to provide critical analyses of standing works. The results of the review are normally in the form of hypothesis or proposal of development new theories and models; arguments of important and/or provocative topics; presenting of the “how to” tips and strategies to improve best practices, and the explanation of the latest expansions in the field (present new viewpoints relating to the salient and developing issues)
There are limitations of narrative literature review: The nature of the method that may be considered too subjective. There is a possibility of misleading in drawing conclusions. These need to be held in consideration.
A literature search was performed for the present study on the lines of searches for an NR. The electronic search included several electronic databases, PubMed, EMBASE ProQuest, Web of Science, ScienceDirect and JSTOR. Cohcrane reviews were also searched and a manual search of texts from the course was undertaken. Search terms used were: ‘mindfulness, ‘competence, and ‘practice’. Also ‘mindfulness+training’ and ‘Fidelity, mindfulness-based cognitive therapy, mindfulness-based program, mindfulness-based stress reduction. The inclusion criteria were: all types of articles, articles published from 1990 onwards. The exclusion criteria were: articles for which full text was not available, were not in English, articles that focused on mindfulness skills of the participant rather than the teacher. From the articles retrieved in the first round of search, additional references were identified by a manual search among the cited references.
Further sections:
- Identify inclusion criteria for studies; Select studies that meet the inclusion criteria;
- Identify themes that emerge from the set of studies, and; Assessment of methodological quality of included reviews
- Results
- Discussion
- Conclusion
- Acknowledgements
- References
- Appendices
References
Baer, R. A. (2015). Mindfulness-Based Treatment Approaches: Clinician’s Guide to Evidence Base and Applications. Academic Press.
Bastian H, Glasziou P, Chalmers I. Seventy-five trials and eleven systematic reviews a day: how will we ever keep up? PLoS Med 2010;7:e1000326.
Biegel, G. M., Shapiro, S. L., Brown, W. K. & Schubert, M. C. (2009). Mindfulness-Based Stress Reduction for the Treatment of Adolescent Psychiatric Outpatients: A Randomized Clinical Trial. Journal of Consulting and Clinical Psychology.
Black, D. S. (2014). Mindfulness and substance use intervention. Substance Use & Misuse, 47(3), 199-201.
Cigolla, F. (2011). A Way of Being: Bringing Mindfulness into Individual Therapy. http://epubs.surrey.ac.uk/24875/2/A%20Way%20of%20Being_Research_report_Publication_Psychotherapy_Research_Brown.pdf
Crane, R. & Kuyken, W. (n.d). Mindfulness-Based Teaching Integrity. University of Exter.
Crane, S. R., Kuyken, W., Williams, G. M. J., Hastings, R. P., Cooper, L. & Fennell, V. J. M. (2011). Competence in Teaching Mindfulness-Based Courses: Concepts, Development and Assessment. Springer Science Business Media
Crane, R. S., Kuyken, W., Williams, J. G., Hastings, R. P., Cooper, L., & Fennell, M. J. V. (2012a). Competence in teaching mindfulness based courses: concepts, development and assessment. Mindfulness, 3(1), 76-84.
Crane, R.S., Soulsby, J.G., Kuyken, W., Williams, J.M.G., Eames, C., Bartley, T., Silverton, S. (2012b). The Bangor, Exeter and Oxford Mindfulness-based Interventions teaching Assessment Criteria (MBI-TAC).
Crane, S. R., Eames, C., Kuyken, W., Hastings, R. P., Williams, J. M. G., Bartley, T., Evans, A., Silverton, S., Soulsby, J. G. & Surawy, C. (2013). Development and Validation of the Mindfulness-Based Interventions: Teaching Assessment Criteria (MBI:TAC). SAGE.
Davis, D. M. & Hayes, J. A. (2010). What are the Benefits of Mindfulness? A Practice Review of Psychotherapy-Related Research. Psychotherapy 48(2). https://www.apa.org/pubs/journals/features/pst-48-2-198.pdf
Francis, A. (2004). Business Mathematics and Statistics. Cengage Learning.
Good Therapy, (n.d). Mindfulness-Based Interventions. http://www.goodtherapy.org/learn-about-therapy/types/mindfulness-based-interventions
Greco, L. A. & Hayes, S. C. (2008). Acceptance & Mindfulness Treatments for Children & Adolescents. New Harbinger Publications.
Groves, P (2015) Mindfulness contextualized: the Buddhist tradition. Royal college of Psychiatrists
Hair, J. F. (2015). Essentials of Business Research Methods. M.E. Sharpe.
Himelstein, S. & Saul, S. (2015). Mindfulness-Based Substance Abuse Treatment for Ad
Cite This Work
To export a reference to this article please select a referencing style below:
Give Yourself The Academic Edge Today
- On-time delivery or your money back
- A fully qualified writer in your subject
- In-depth proofreading by our Quality Control Team
- 100% confidentiality, the work is never re-sold or published
- Standard 7-day amendment period
- A paper written to the standard ordered
- A detailed plagiarism report
- A comprehensive quality report
Essay Writing Service
Essay Writing
Service
AED558.00
Approximate costs for Undergraduate 2:2
1000 words
7 day delivery
Order An Essay TodayDelivered on-time or your money back
1858 reviews